Conquering pain
Why is cancer sometimes associated with pain?
It is a paradox, but pain is rarely a symptom of cancer in the early stages. Because tumours are made up of tissue very closely similar to the normal tissues of the body, the presence of a tumour does not usually signal alarm until it has progressed quite significantly. For this reason many cancers are not diagnosed until the later stages, and malignant breast lumps are rarely painful, unless there is surrounding inflammation.
However, pain is a common problem in patients with metastatic cancer. When a tumour forms in a distant organ such as bone or liver or lung, as it grows it causes tension on the lining of those organs. The lining of organs like the liver and the bone is a thin membrane rather like thin plastic, or "Glad-Wrap". It contains many sensitive nerve endings, and as it gets stretched it causes messages that go to the brain and tell the brain that something is wrong. These messages are received as pain signals. Sometimes the tumour presses directly on nerves giving rise to what is called “neuropathic” pain. Sometimes the body produces inflamed tissue around the tumour as part of its attempt to control and fight the tumour. Just as a boil or an abscess is painful, so this inflammatory process may also cause pain.
Of course, the best way of stopping the problem is to get rid of the tumour, and that is always our primary goal. There are many ways of doing this. It might involve the use of chemotherapy, or hormone therapy. Sometimes it involves removing the lump surgically. Sometimes the tumour can be reduced in size by using radiotherapy.
Often however, it takes some time before any of these methods of cancer therapy can be effective. It is therefore very frequently necessary to use quite strong painkillers while we are awaiting the full effects of anti-cancer treatment.
Good Rules for Pain Control
Remember that nowadays we are able to control cancer pain in more than 90 per cent of cases, but doing so requires your strict co-operation.
Remember, there are no medals for putting up with pain. Keep in mind always that you are wasting energy if you are tolerating pain, and that this energy would be much better conserved and used in the important battle - fighting the cancer.
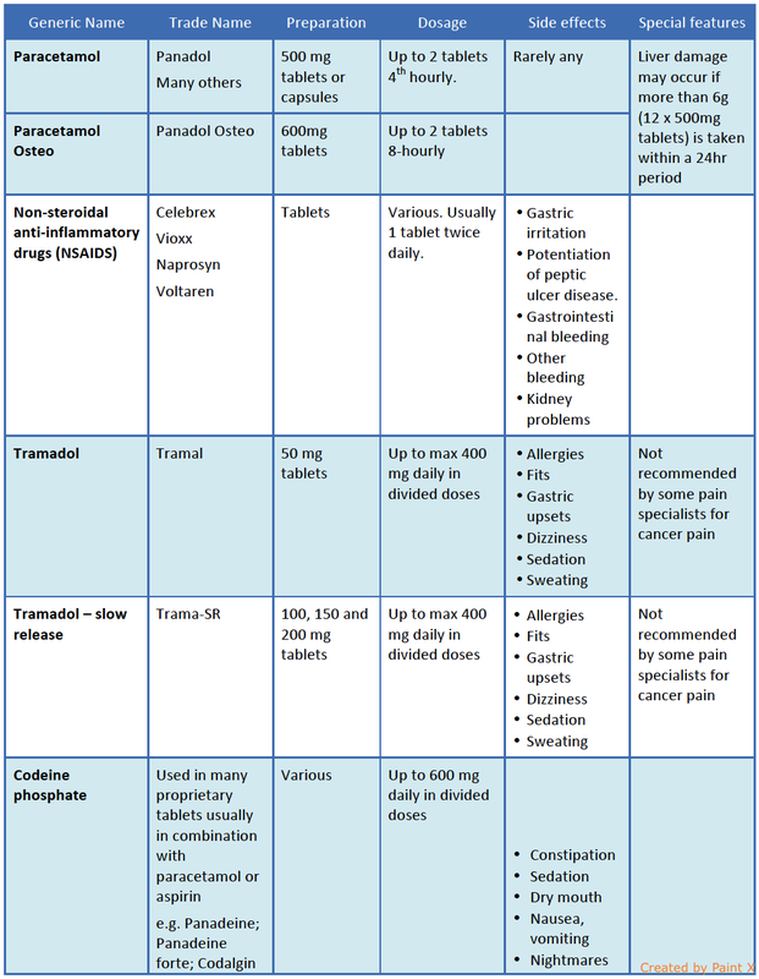
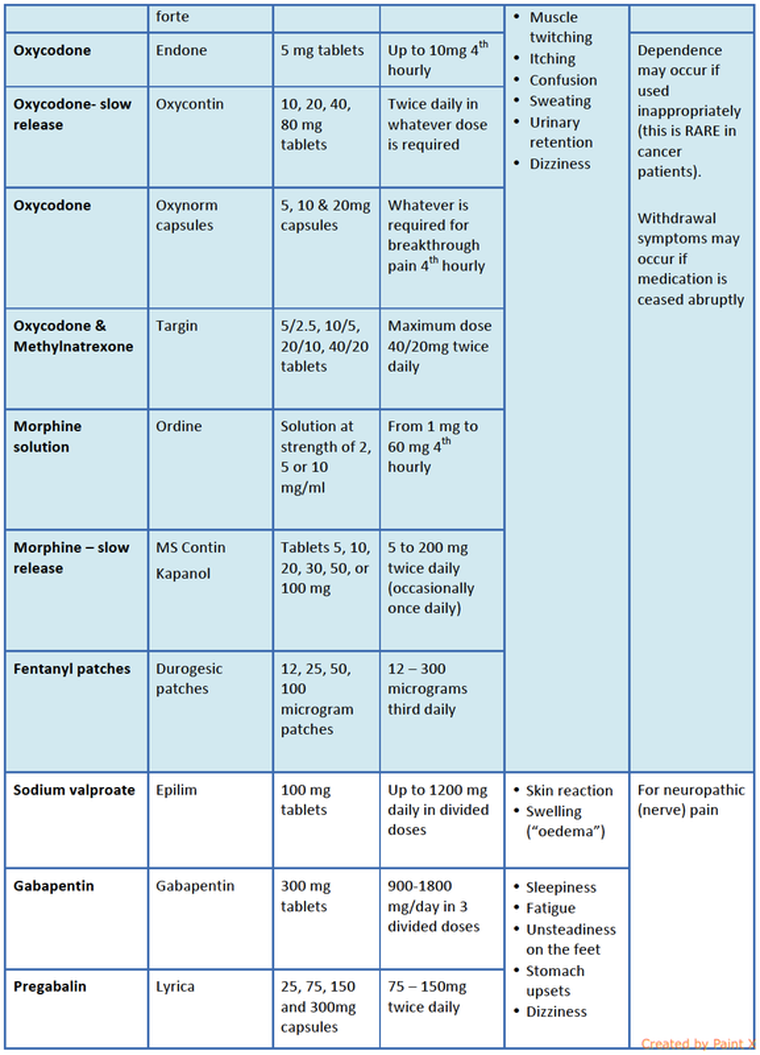
Some of the drugs commonly in use for control of pain are shown in the Table below.
The following are the most important rules about treating pain when cancer is the cause:
1. Take pain-killers regularly.
Pain medication should be taken regularly as instructed by your doctor or nurse, strictly by the clock, whether or not the pain is present. This is the rule that is most commonly broken by patients. People seem to think that it is better to wait until the pain is bad. They think that the pain medication might stop being effective, or that they might “get used to the medication”, or that perhaps, it might not work later on in their illness when they might need it more. All of these commonly held beliefs are completely wrong. Most simple painkillers, like paracetamol, have a relatively short time span of action, usually around four hours. In order to get good control of pain, it is important to think of forming a barrier in the blood stream by keeping a constant level of pain medication present. If you allow peaks and troughs to develop in the level of painkiller, you will never get good pain control, and in fact, you may end up developing tolerance to the pain medication much more so than you would if you were to take the medication strictly by the clock, every four hours. You will not get used to the medication, you will not get addicted to it, and it will not wear off. People who take their pain medication strictly according to these instructions very rarely require constantly increasing doses. It is true that everybody is different and everybody metabolises pain medications at a different rate. This means that each individual has a particular dose level of each pain medication that is fairly unique. Whereas some people may only need a very small dose, others might need ten times that dose.
2. Listen to a professional
Many people get into trouble by adjusting doses too quickly, or perhaps stopping the medication altogether, because they develop some side-effects like constipation or nausea. Others find that they are a little sedated or nauseated when they first start stronger pain medication and they might be tempted to reduce the dose. It is most important that you try to stick to the doses recommended by your doctor and nursing staff, who will probably have arranged for you to be in contact with them around 48 hours after you start medication. This is often a good time to modify the dose, but strictly only under medical or nursing supervision. Do not be discouraged if you have a little nausea or sedation during the early stages of taking stronger analgesics like morphine or oxycodone. These effects are common, and they usually wear off quite quickly, leaving the positive effects of pain control without major side-effects.
3. Don’t underestimate simple analgesics
Commonly, pain control is commenced with a simple analgesic drug like paracetamol, or a combination of paracetamol with codeine. This is given in a strict fourth-hourly regime. If pain levels continue, we may introduce the drug oxycodone. If this fails, morphine is commonly introduced. This gradual escalation of strength in pain-killers is called the “analgesic pyramid”.
Don’t underestimate paracetamol. It is a very effective pain-killer, and it is almost entirely free of side-effects. It MUST be taken regularly, though, usually one-to-two 500 mg tablets every four hours. Longer acting forms are also available which are taken three times daily. Paracetamol as a base is really good for bone pain and also helps to increase the effectiveness of the other stronger painkillers such as oxycodone.
4. Don’t be afraid of the opiate analgesics: oxycodone and morphine.
Most of our strong pain-killers are still derived from opium. These drugs include codeine, oxycodone and morphine. Heroine used to be used in control of strong pain, but has been shown to be no more effective than morphine. Many people are afraid about taking morphine. They think that they might “get used to the medication”, or that perhaps, it might not work later on in their illness when they might need it more. They also think that they will become addicted to the morphine and never be able to stop taking it. Others believe that once they are on morphine that, somehow, they are on a relentlessly downhill path. All of these commonly held beliefs are completely wrong. If you are taking it for pain, you will not get used morphine, you will not get addicted to it, and it will not wear off. People who take their pain medication strictly according to medical instructions very rarely require constantly increasing doses.
Initially, morphine is given once every four hours. Once it used to be thought that morphine had to be given by injection. In fact, the drug is well absorbed from the stomach. It is usually taken as a liquid. Your oncology nurse will show you how to measure out the correct amount of liquid morphine. If you wish, you can measure out all of the doses for one day into separate plastic medicine glasses, and if you prefer, the morphine can be diluted with orange juice. It is important if you are going out that you take your dose with you. Although we recommend that you take each dose strictly by the clock every four hours, it is not necessary to wake yourself in the middle of that night if you are sleeping soundly. Some people find that it helps them to take a double dose on retiring, and that is perfectly safe.
One of the that most important developments in if pain control in the past ten years has been the development and refinement of long acting painkillers. These drugs can be taken just twice daily, instead of once every four hours. Sometimes, they may be taken just once daily. Obviously, this is a major improvement in convenience. In addition to convenience, these longer acting analgesics sometimes have fewer side-effects than the older short acting ones.
It is usually wise to start pain control using the older short acting analgesics. There are several reasons for this. Most importantly, it allows your doctors and nurses to titrate the dose of painkiller to your precise individual needs. Every individual has a different requirement for analgesic dose, and of course, pain levels differ from circumstance to circumstance.
In special cases we may use certain painkillers instead of morphine and some of these are listed in the table. Often these are best prescribed by an expert in control of cancer pain – usually a Palliative Care Specialist, or the Chronic Pain Team in a major hospital.
5. Get used to multiple medications.
It is commonly necessary to use a combination of medicines to get good pain control. Many patients have a natural aversion to this. Most patients say to me things like, “I’m not one for taking tablets, doc!”. But it is essential that some of these ingrained reactions are overcome if good pain control is to be achieved. For example, paracetamol can actually assist the action of stronger pain killers like morphine, a phenomenon known as “synergy”. It is also common to add drugs like anti-arthritis or anti-inflammatory medication. This may consist of so-called non-steroidal anti-inflammatories, “NSAIDS” like Naprosyn, Celebrex or Voltaren, or corticosteroids, like prednisone or dexamethasone (“Decadron”). Sometimes antidepressant medication is added, like nortryptaline (“Tryptanol”). This is not necessarily because depression is present, but because it assists in suppression of pain signals. Tranquilisers like diazepam (“Valium”) are also sometimes used. As nearly all strong painkillers cause constipation most patients will also require regular laxatives. Do not be surprised if you need to take four or five different medications to get good pain control.
Side-effects of pain-killers
Constipation
Constipation occurs with nearly all strong painkillers. This is because the painkillers inhibit nerve supply to the bowel and inhibit contraction of the intestine. Constipation is nearly always very readily controlled using laxatives like senna (“Senokot”), (which stimulates contraction of the bowel), Coloxyl (which softens the bowel motion), and bulking agents, like Movicol and Normacol. These should be taken regularly while strong analgesics are prescribed, unless diarrhoea occurs.
Sedation
Sedation often occurs within the first 24-48 hours of taking a new analgesic, but may well settle after that as your body acclimatizes. It is usually possible to obtain good long-term pain control without severe sedation. If one particular medication causes a lot of sedation, don't despair, there are many other different flavours.
Dry Mouth
This is a common side-effect and one that is quite difficult to treat. Carry water with you – often a squeeze bottle is helpful. Dry mouth sprays and gels are also readily available to buy at the chemist.
Nausea.
Nausea often occurs within the first 24-48 hours of taking a new analgesic, but may well settle after that as your body acclimatizes. Simple anti-nausea drugs like “Stemetil” or “Maxolon” may be useful during this period. Some people are genuinely intolerant to certain analgesics and in these special situations other analgesics, like Fentanyl may be helpful.
Difficulty concentrating, confusion
Itching and skin rash.
Muscle twitching
This is usually a sign that the dose may be too high.
Hallucinations.
Typically these involve seeing ugly, deformed faces, or animals climbing on the bed-curtains. This is usually a sign that the dose may be too high.
Nightmares.
Urinary retention
This may be a special problem for men with prostate problems. Sometimes simple things may help, like running a tap while you are trying to pass urine, or passing urine in the shower. Don’t worry! Urine is perfectly sterile!
Sweating
Dizziness
This may be due to lowering of the blood pressure and it may be necessary to reduce the doses of other blood pressure medication, strictly under medical advice
What about marijuana?
Some prominent public figures have argued that marijuana should be legalised for cancer patients because of its effectiveness in pain control. For a discussion of this subject, click here.
Commonly used pain-killers
It is a paradox, but pain is rarely a symptom of cancer in the early stages. Because tumours are made up of tissue very closely similar to the normal tissues of the body, the presence of a tumour does not usually signal alarm until it has progressed quite significantly. For this reason many cancers are not diagnosed until the later stages, and malignant breast lumps are rarely painful, unless there is surrounding inflammation.
However, pain is a common problem in patients with metastatic cancer. When a tumour forms in a distant organ such as bone or liver or lung, as it grows it causes tension on the lining of those organs. The lining of organs like the liver and the bone is a thin membrane rather like thin plastic, or "Glad-Wrap". It contains many sensitive nerve endings, and as it gets stretched it causes messages that go to the brain and tell the brain that something is wrong. These messages are received as pain signals. Sometimes the tumour presses directly on nerves giving rise to what is called “neuropathic” pain. Sometimes the body produces inflamed tissue around the tumour as part of its attempt to control and fight the tumour. Just as a boil or an abscess is painful, so this inflammatory process may also cause pain.
Of course, the best way of stopping the problem is to get rid of the tumour, and that is always our primary goal. There are many ways of doing this. It might involve the use of chemotherapy, or hormone therapy. Sometimes it involves removing the lump surgically. Sometimes the tumour can be reduced in size by using radiotherapy.
Often however, it takes some time before any of these methods of cancer therapy can be effective. It is therefore very frequently necessary to use quite strong painkillers while we are awaiting the full effects of anti-cancer treatment.
Good Rules for Pain Control
Remember that nowadays we are able to control cancer pain in more than 90 per cent of cases, but doing so requires your strict co-operation.
Remember, there are no medals for putting up with pain. Keep in mind always that you are wasting energy if you are tolerating pain, and that this energy would be much better conserved and used in the important battle - fighting the cancer.
Some of the drugs commonly in use for control of pain are shown in the Table below.
The following are the most important rules about treating pain when cancer is the cause:
1. Take pain-killers regularly.
Pain medication should be taken regularly as instructed by your doctor or nurse, strictly by the clock, whether or not the pain is present. This is the rule that is most commonly broken by patients. People seem to think that it is better to wait until the pain is bad. They think that the pain medication might stop being effective, or that they might “get used to the medication”, or that perhaps, it might not work later on in their illness when they might need it more. All of these commonly held beliefs are completely wrong. Most simple painkillers, like paracetamol, have a relatively short time span of action, usually around four hours. In order to get good control of pain, it is important to think of forming a barrier in the blood stream by keeping a constant level of pain medication present. If you allow peaks and troughs to develop in the level of painkiller, you will never get good pain control, and in fact, you may end up developing tolerance to the pain medication much more so than you would if you were to take the medication strictly by the clock, every four hours. You will not get used to the medication, you will not get addicted to it, and it will not wear off. People who take their pain medication strictly according to these instructions very rarely require constantly increasing doses. It is true that everybody is different and everybody metabolises pain medications at a different rate. This means that each individual has a particular dose level of each pain medication that is fairly unique. Whereas some people may only need a very small dose, others might need ten times that dose.
2. Listen to a professional
Many people get into trouble by adjusting doses too quickly, or perhaps stopping the medication altogether, because they develop some side-effects like constipation or nausea. Others find that they are a little sedated or nauseated when they first start stronger pain medication and they might be tempted to reduce the dose. It is most important that you try to stick to the doses recommended by your doctor and nursing staff, who will probably have arranged for you to be in contact with them around 48 hours after you start medication. This is often a good time to modify the dose, but strictly only under medical or nursing supervision. Do not be discouraged if you have a little nausea or sedation during the early stages of taking stronger analgesics like morphine or oxycodone. These effects are common, and they usually wear off quite quickly, leaving the positive effects of pain control without major side-effects.
3. Don’t underestimate simple analgesics
Commonly, pain control is commenced with a simple analgesic drug like paracetamol, or a combination of paracetamol with codeine. This is given in a strict fourth-hourly regime. If pain levels continue, we may introduce the drug oxycodone. If this fails, morphine is commonly introduced. This gradual escalation of strength in pain-killers is called the “analgesic pyramid”.
Don’t underestimate paracetamol. It is a very effective pain-killer, and it is almost entirely free of side-effects. It MUST be taken regularly, though, usually one-to-two 500 mg tablets every four hours. Longer acting forms are also available which are taken three times daily. Paracetamol as a base is really good for bone pain and also helps to increase the effectiveness of the other stronger painkillers such as oxycodone.
4. Don’t be afraid of the opiate analgesics: oxycodone and morphine.
Most of our strong pain-killers are still derived from opium. These drugs include codeine, oxycodone and morphine. Heroine used to be used in control of strong pain, but has been shown to be no more effective than morphine. Many people are afraid about taking morphine. They think that they might “get used to the medication”, or that perhaps, it might not work later on in their illness when they might need it more. They also think that they will become addicted to the morphine and never be able to stop taking it. Others believe that once they are on morphine that, somehow, they are on a relentlessly downhill path. All of these commonly held beliefs are completely wrong. If you are taking it for pain, you will not get used morphine, you will not get addicted to it, and it will not wear off. People who take their pain medication strictly according to medical instructions very rarely require constantly increasing doses.
Initially, morphine is given once every four hours. Once it used to be thought that morphine had to be given by injection. In fact, the drug is well absorbed from the stomach. It is usually taken as a liquid. Your oncology nurse will show you how to measure out the correct amount of liquid morphine. If you wish, you can measure out all of the doses for one day into separate plastic medicine glasses, and if you prefer, the morphine can be diluted with orange juice. It is important if you are going out that you take your dose with you. Although we recommend that you take each dose strictly by the clock every four hours, it is not necessary to wake yourself in the middle of that night if you are sleeping soundly. Some people find that it helps them to take a double dose on retiring, and that is perfectly safe.
One of the that most important developments in if pain control in the past ten years has been the development and refinement of long acting painkillers. These drugs can be taken just twice daily, instead of once every four hours. Sometimes, they may be taken just once daily. Obviously, this is a major improvement in convenience. In addition to convenience, these longer acting analgesics sometimes have fewer side-effects than the older short acting ones.
It is usually wise to start pain control using the older short acting analgesics. There are several reasons for this. Most importantly, it allows your doctors and nurses to titrate the dose of painkiller to your precise individual needs. Every individual has a different requirement for analgesic dose, and of course, pain levels differ from circumstance to circumstance.
In special cases we may use certain painkillers instead of morphine and some of these are listed in the table. Often these are best prescribed by an expert in control of cancer pain – usually a Palliative Care Specialist, or the Chronic Pain Team in a major hospital.
5. Get used to multiple medications.
It is commonly necessary to use a combination of medicines to get good pain control. Many patients have a natural aversion to this. Most patients say to me things like, “I’m not one for taking tablets, doc!”. But it is essential that some of these ingrained reactions are overcome if good pain control is to be achieved. For example, paracetamol can actually assist the action of stronger pain killers like morphine, a phenomenon known as “synergy”. It is also common to add drugs like anti-arthritis or anti-inflammatory medication. This may consist of so-called non-steroidal anti-inflammatories, “NSAIDS” like Naprosyn, Celebrex or Voltaren, or corticosteroids, like prednisone or dexamethasone (“Decadron”). Sometimes antidepressant medication is added, like nortryptaline (“Tryptanol”). This is not necessarily because depression is present, but because it assists in suppression of pain signals. Tranquilisers like diazepam (“Valium”) are also sometimes used. As nearly all strong painkillers cause constipation most patients will also require regular laxatives. Do not be surprised if you need to take four or five different medications to get good pain control.
Side-effects of pain-killers
Constipation
Constipation occurs with nearly all strong painkillers. This is because the painkillers inhibit nerve supply to the bowel and inhibit contraction of the intestine. Constipation is nearly always very readily controlled using laxatives like senna (“Senokot”), (which stimulates contraction of the bowel), Coloxyl (which softens the bowel motion), and bulking agents, like Movicol and Normacol. These should be taken regularly while strong analgesics are prescribed, unless diarrhoea occurs.
Sedation
Sedation often occurs within the first 24-48 hours of taking a new analgesic, but may well settle after that as your body acclimatizes. It is usually possible to obtain good long-term pain control without severe sedation. If one particular medication causes a lot of sedation, don't despair, there are many other different flavours.
Dry Mouth
This is a common side-effect and one that is quite difficult to treat. Carry water with you – often a squeeze bottle is helpful. Dry mouth sprays and gels are also readily available to buy at the chemist.
Nausea.
Nausea often occurs within the first 24-48 hours of taking a new analgesic, but may well settle after that as your body acclimatizes. Simple anti-nausea drugs like “Stemetil” or “Maxolon” may be useful during this period. Some people are genuinely intolerant to certain analgesics and in these special situations other analgesics, like Fentanyl may be helpful.
Difficulty concentrating, confusion
Itching and skin rash.
Muscle twitching
This is usually a sign that the dose may be too high.
Hallucinations.
Typically these involve seeing ugly, deformed faces, or animals climbing on the bed-curtains. This is usually a sign that the dose may be too high.
Nightmares.
Urinary retention
This may be a special problem for men with prostate problems. Sometimes simple things may help, like running a tap while you are trying to pass urine, or passing urine in the shower. Don’t worry! Urine is perfectly sterile!
Sweating
Dizziness
This may be due to lowering of the blood pressure and it may be necessary to reduce the doses of other blood pressure medication, strictly under medical advice
What about marijuana?
Some prominent public figures have argued that marijuana should be legalised for cancer patients because of its effectiveness in pain control. For a discussion of this subject, click here.
Commonly used pain-killers