Now my treatment’s over, what now?
You would think that once someone had come to the end of chemotherapy and radiotherapy and surgery for the treatment of early breast cancer that they would simply crack open a bottle of champagne, and delightedly rush away hoping never to see those doctors again! The surprising thing is that, in fact, many many women find this a very difficult time and have a sensation that they are being abandoned from a safe world of planned, continuing treatments and medical reviews, and that now, suddenly, they are on their own.
This is a time when many anxieties still find their way to the surface:
I will try to answer each of these questions, but keep in mind the overriding fact: the vast majority of women with early breast cancer do not suffer recurrence. As your body returns to normal after your treatment, your hair re-grows, your body rhythms return to normal, and your confidence is regained, and as it becomes longer and longer in time since that distant treatment, your inner strength and certainty will increase exponentially.
Can we do tests to ensure that the cancer has all gone?
One of the Holy Grails of Cancer Research is to find simple blood tests or urine tests that would tell us reliably and with 100 per cent accuracy if there are just a few cancer cells in the body. Unfortunately, with the possible exception of the "PSA" test for prostate cancer, there are no such tests. There are some blood tests promoted for this use in following women who have had breast cancer. These include the CA 15.3 and CA 27.29 which are blood tests and are used by some oncologists in Australia and the US. However, the current guidelines of the American Society for Clinical Oncology advise against their use because there are too many false positives and false negatives.
Similarly, the use of regular imaging investigations (such as X-rays, CT scans, bone scans, and PET scans) have been investigated in the follow-up of young women with early breast cancer. Again, current advice in Australia is that these tests not be used unless there is some persistent, progressive, and unusual symptom which deserves investigation. There is no current evidence that picking up secondary breast cancer before such symptoms have become obvious leads to better management. There are a number of very useful treatments for secondary breast cancer, but these are just as effective if used when the problem is obvious, as if they were used when there was just some microscopic problem picked up only on some sensitive scan.
Often, when scans are performed, they show up problems that have nothing to do with the breast cancer and which cannot be diagnosed because the lesions are too small to be localised and to biopsy. This situation, which is not at all uncommon for oncologists, (who have patients referred having had scans done, perhaps at the patient’s insistence, by their general practitioner or by another doctor), is simply managed by advising the patient to sit tight and have this scans repeated in three or six months time. This just results in unnecessary anxiety for the patient and her family.
What are the goals of medical follow-up?
The goals of follow-up after your treatment is complete include:
With current treatment protocols, the rate of recurrence of cancer in the treated breast is 1–2 per cent per annum and 1 per cent after mastectomy. For women who have had mastectomy, most recurrences will be detected by clinical examination alone. For women who have had breast conserving surgery (lumpectomy and radiotherapy), many will be detected by regular mammography.
The usual treatments for local recurrence are surgery and radiotherapy, and these are more effective if used in the earliest phases of recurrence. Therefore much of the focus of our follow-up is directed at detecting local recurrence. That is probably best done by an experienced breast clinician, often your original surgeon and/or radiation oncologist.
A history of breast cancer increases the risk of a second, separate, quite new primary breast cancer. This risk is approximately 1% per annum. That is, out of every 100 women who have had one breast cancer, one will develop a new primary breast cancer each year. Half of these will occur in the opposite breast. Accordingly, regular (at least annual) mammography is strongly recommended.
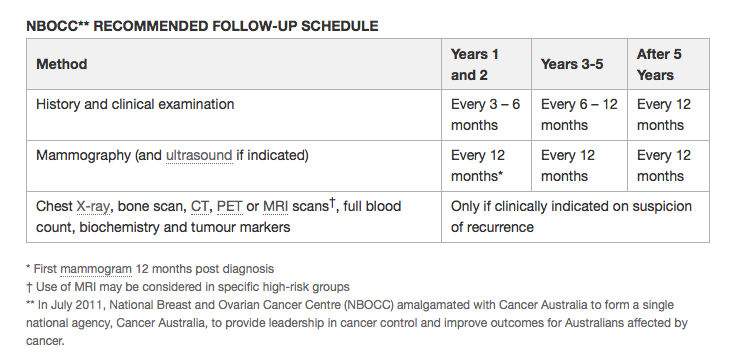
Australian Guidelines for Follow-up
The Australian Guidelines for follow-up after early breast cancer are shown in the table
This is a time when many anxieties still find their way to the surface:
- How will I know if the cancer has come back?
- I am having some aches in my back and in my joints, does this mean that I have cancer in the bones?
- My breast feels hard after the radiotherapy; does this mean that the cancer is back?
- Why can't the doctors do blood tests and scans at regular intervals to reassure me that I am clear of cancer?
- How do we know that the chemotherapy and hormone therapy was effective?
I will try to answer each of these questions, but keep in mind the overriding fact: the vast majority of women with early breast cancer do not suffer recurrence. As your body returns to normal after your treatment, your hair re-grows, your body rhythms return to normal, and your confidence is regained, and as it becomes longer and longer in time since that distant treatment, your inner strength and certainty will increase exponentially.
Can we do tests to ensure that the cancer has all gone?
One of the Holy Grails of Cancer Research is to find simple blood tests or urine tests that would tell us reliably and with 100 per cent accuracy if there are just a few cancer cells in the body. Unfortunately, with the possible exception of the "PSA" test for prostate cancer, there are no such tests. There are some blood tests promoted for this use in following women who have had breast cancer. These include the CA 15.3 and CA 27.29 which are blood tests and are used by some oncologists in Australia and the US. However, the current guidelines of the American Society for Clinical Oncology advise against their use because there are too many false positives and false negatives.
Similarly, the use of regular imaging investigations (such as X-rays, CT scans, bone scans, and PET scans) have been investigated in the follow-up of young women with early breast cancer. Again, current advice in Australia is that these tests not be used unless there is some persistent, progressive, and unusual symptom which deserves investigation. There is no current evidence that picking up secondary breast cancer before such symptoms have become obvious leads to better management. There are a number of very useful treatments for secondary breast cancer, but these are just as effective if used when the problem is obvious, as if they were used when there was just some microscopic problem picked up only on some sensitive scan.
Often, when scans are performed, they show up problems that have nothing to do with the breast cancer and which cannot be diagnosed because the lesions are too small to be localised and to biopsy. This situation, which is not at all uncommon for oncologists, (who have patients referred having had scans done, perhaps at the patient’s insistence, by their general practitioner or by another doctor), is simply managed by advising the patient to sit tight and have this scans repeated in three or six months time. This just results in unnecessary anxiety for the patient and her family.
What are the goals of medical follow-up?
The goals of follow-up after your treatment is complete include:
- The early detection of local recurrence in the breast itself, on the chest wall, or in local lymph glands
- Screening for a new primary breast cancer, in the same, or opposite breast
- Detection of treatment-related side-effects, like radiation damage to the lung, swelling of the arm (lymphoedema), shoulder problems, problems with menopause, or problems with tamoxifen.
- Provision of psychosocial support
- Identification of family history
With current treatment protocols, the rate of recurrence of cancer in the treated breast is 1–2 per cent per annum and 1 per cent after mastectomy. For women who have had mastectomy, most recurrences will be detected by clinical examination alone. For women who have had breast conserving surgery (lumpectomy and radiotherapy), many will be detected by regular mammography.
The usual treatments for local recurrence are surgery and radiotherapy, and these are more effective if used in the earliest phases of recurrence. Therefore much of the focus of our follow-up is directed at detecting local recurrence. That is probably best done by an experienced breast clinician, often your original surgeon and/or radiation oncologist.
A history of breast cancer increases the risk of a second, separate, quite new primary breast cancer. This risk is approximately 1% per annum. That is, out of every 100 women who have had one breast cancer, one will develop a new primary breast cancer each year. Half of these will occur in the opposite breast. Accordingly, regular (at least annual) mammography is strongly recommended.
Australian Guidelines for Follow-up
The Australian Guidelines for follow-up after early breast cancer are shown in the table